
Why Covid Can Never Be 'Just A Cold'
The science


The covid-is-just-a-cold myth has made its way deep into society.
I've certainly heard it from friends and family.
You probably have too.
Some experts have pushed this line because the virus that causes covid - Sarscov2 - is a coronavirus, and some other coronaviruses cause colds.
This is an incredibly bad simplification. It is unscientific. It is dangerous. And it is doing real harm to people’s ability to understand what covid is and why they should do more to avoid it.
The science of this is so important, so I’ve decided to revise and update an article I wrote about this last summer, drawing on the latest research.
But before we get to the science.
I’ve said it many times before, and it bears repeating again and again: most people didn’t wake up one day and decide to think about covid like a cold. People didn’t go from being happy to isolate, test, mask, lock down, to being chill about coexisting with this virus.
The normalising process wasn’t organic, it was engineered.
A particularly egregious example of hegemonic covid-as-cold propaganda originated in the UK.
On 28th December, 2021, Paul Hunter, a microbiologist at the University of East Anglia, appeared on the BBC's popular live breakfast TV show and, advocating the end of covid isolation rules, said:
‘Ultimately, we’re going to have to let people who are positive with Covid go about their normal lives as they would do with any other cold. Covid will become just another cause of the common cold.”
This quote was picked up by media from the The Guardian to Fox News to the Telegraph, to WeLoveTrump.com (yes, really) and everything in between. I documented it here.
This was just one occasion among many where dodgy scientists, via dodgy reporters, encouraged us to think about covid as being like a cold. In December 2022, The Atlantic asked Is Covid A Common Cold Yet? The idea that soon Sarscov2 would become a different virus to that scary one from 2020 was pushed continually.
The reality is covid can never, ever be a common cold.
The mistake The Atlantic makes is equating the symptoms with the disease.
If covid is here in three hundred years, it won’t be a cold.
Why? Because Sarscov2 infects cells in the human body in a very different way to any other virus that causes a cold.
Coronaviruses and rhinoviruses are the two primary viruses that cause common colds. There are at least 160 recognised rhinovirus types, and just seven recognised coronaviruses that infect humans.
These viruses enter the body by binding to cells in the nose, infecting primarily the upper respiratory tract, and, more rarely, the lower respiratory tract (lungs) as well.
The thing is, among the many recognised rhinoviruses, the seven coronaviruses (and the handful of flu strains) there are only three that attach themselves to an enzyme found not just in the respiratory tract, but in cells across the body – and Sarscov2 is one of them.
The enzyme is known as ACE2, and it is pumped out, or, to use the scientific term, expressed, by cells that live in pretty much all of our organs.
As this paper puts it: “ACE2 is abundantly expressed in a variety of cells residing in many different human organs.”
From our kidneys to our livers to our hearts to brains.
This is a problem. Maybe you can see why.
Most genuine cold-causing viruses only have a few paths of entry and are generally restricted to the upper and lower airways.
When it comes to Sarscov2 however, your body is like a giant hotel with hundreds of doors. And as soon as it rocks up, the virus has a way of unlocking these doors (more on that later) and strolling through them into the organs that lie behind.
This is why, once the virus has established itself in your body, it can cause heart attacks, liver damage, kidney damage, gut damage, thyroid damage, brain damage and on and on.
Heart attack spikes over the first three years of the pandemic correlated almost perfectly with covid waves.
All-cause excess deaths in young adults also correlated uncannily with covid waves, as you can see here.

But back to those other two coronaviruses that use ACE2 to infect the body: Sarscov1 and a coronavirus known as NL63.
The first Sars caused a devastating outbreak in 2002-2003. Despite infecting fewer than 10,000 people, it caused close to 1,000 deaths. Scientists pegged its mortality rate at around 10%, and nearer 50% for the over 60s. Its use of ACE2 was one of the primary reasons. It was ended by aggressive test and tracing, along with strict quarantine rules. It was also less transmissible than Sarscov2.
How about NL63? NL63 was only discovered in 2004, so the science on it is less than 20 years old. Despite using ACE2, it causes less serious disease than Sars 1 and 2 for another reason, which we’ll get to.
The truth is, until recently, coronaviruses had been disproportionally under-studied compared to, say, influenza viruses. One reason for this is that there was a general assumption that the next pandemic would involve an influenza virus, rather than a coronavirus.
Oooops.
That is now changing. And more answers are being found. More studies on the ACE2 connection with organ damage is yielding those answers.
As is the study of the envelope protein.
A virus is made up of different proteins. A coronavirus is made up of four main types of proteins. One of these is the envelope protein. When you are infected with a coronavirus, the envelope protein interacts with a specific human protein called PALS-1.
What researchers are now discovering is that the stability of the interaction, or binding, between these two proteins is crucial to the ability of a coronavirus to cause disease.
The thing about the envelope protein of the Sarscov2 coronavirus is that it is longer and more flexible than the envelope protein of all the other coronaviruses, including NL63. This means it can mould itself, like a piece of putty, to fit more snugly around the human protein.
So while NL63, like Sarscov1 and 2, uses ACE2 to infect us, unlike a Sars virus it is all thumbs when trying to interact with PALS-1.
So, if the envelope protein of NL63 and other coronaviruses are all thumbs, trying their best to force a square peg into a round keyhole, the envelope protein of Sars-cov2 is a bit like a spider key for all those doors leading to the organs in your body.
But what about the 160 different rhinoviruses, which cause more than 50% of all common colds?
They have no envelope protein!
Rhinoviruses don’t have thumbs, let alone fingers. This lack of dexterity means their ability to infect cells across your body and cause severe disease is severely blunted.
So no. Covid is not a cold yet.
And it never can be.
The question itself is framed all wrong.
The fundamental mechanisms underlying how Sarscov2 causes disease is never going to change.
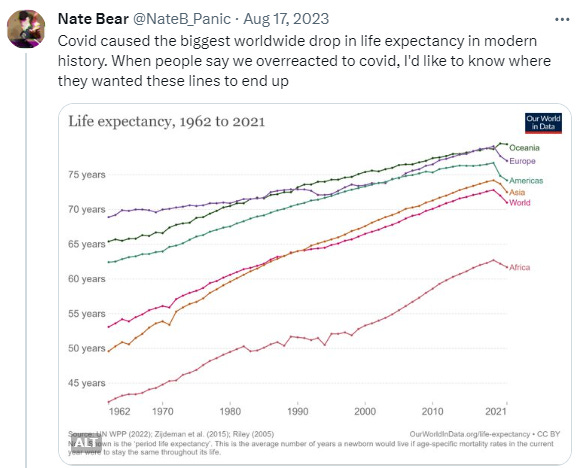
It didn’t crash life expectancy on every continent on Earth because it’s just a cold.
It is the virus that it is, and it will stay that way.
Vaccines have not turned covid into a common cold.
Multiple infections will not turn covid into a common cold.
Antibodies and T-cell responses (a longer lasting line of defence against pathogens than antibodies) from vaccination and infection do mean we are not naïve to it any longer, which, along with many of the most vulnerable already being killed by it, has brought deaths and hospitalisations down.
But the virus is constantly mutating past antibodies generated from encounters with older strains, and it is never going to stop using ACE2 to infect us. The Sars envelope protein is never going to change. The virus continues to kill and disable every single day.
In the US nearly 2,400 people died of covid last week. The risk of long-term effects from covid after the acute phase has passed is close to 1 in 10 in the vaccinated and 1 in 4 in the unvaccinated.
The implications of a virus that can never become a cold are being articulated by researchers.
One implication is a significant and prolonged rise in heart attacks. Researchers have recently documented persistent infection of the heart in recovered covid patients (because the virus accesses the heart via ACE2), and as a result they suggested a “heart failure pandemic” is looming.
Another implication, according to a neuroscientist studying covid, is ‘a generation of babies being born with long covid.’ It is increasingly being shown that a pregnant mother infected with Sarscov2 can pass on the virus to her unborn baby, and this can affect fetal brain development. Long covid is increasingly recognised as a neurological disease, its effects rippling out from the brain across the body.
Another is viral persistence, with more research pointing to the likelihood that the virus is not fully cleared from the body even in those who have seemingly recovered after an infection. This can lead to ongoing inflammation, often a trigger for other conditions.
This inflammation, alongside the neurological impacts, lie in large part behind long covid, a catch-all term for a large basket of post acute infection conditions, from the debilitating, such as myalgic encephalomyelitis, which leaves sufferers bedbound and reliant on 24/7 care, to the more manageable but chronic, such as persistent headaches, nervous system disruption, thyroid and kidney injury/disease.
Covid can also mess up your immune system and turn it against you, provoking conditions such as diabetes and rheumatoid arthritis. The risk of a new onset autoimmune condition after covid is high, a large study last year concluded.
A new lie has recently begun to circulate: that most people who are going to get long covid have got it/had it. No research supports this. On the contrary. The most solid research suggests repeat infections raise your risk of long covid.
This is all heavy information.
It’s not pleasant to learn.
It demands reaction.
So what can we do? We need to demand decent masks (N95 in US, FFP2-3 in Europe) in hospitals and public transport at a minimum. We need to demand clean indoor air, especially in places known to drive transmission like hospitals, schools, colleges and universities. If you live in a country that no longer allows covid vaccines for the under 60s, you need to demand them. We need to demand access to better vaccines that target a broader part of the Sarscov2 virus and are more resistant against mutations, like Novavax.
For people to even know to demand these things, we need to spread the reality about what covid still is.
So if you found this useful, maybe someone else you know would too. Please share.
Because if we keep being sold the lie that covid is just a cold, and if people keep buying it, we're going to end up in ever-deeper trouble, individually, and as a society.
Thanks for this very good ‘reader-friendly’ essay....unfortunately people choose to believe the ‘misinformation’. We are all lemings heading collectively for the cliff. Unless science can find a way to stop this virus and to stop its ‘Long Covid’ impacts I fear the future of humanity. Thanks for this! I wish SARS-CoV-2 was a cold but know it is not...I hate this virus!!
My first bout with Covid gave me a year of severe gastrointestinal problems. It rendered my GI tract pretty much unable to operate. I had severe acid damage from esophagus to the duodenum. I also ended up with high blood pressure. Did not have that or any stomach issues prior to Covid infection.
And most recently my 81 year old mom was in the hospital for a blood infection. Zero hospital staff wore masks of any kind. My mom caught Covid in the hospital but none of the staff even noticed. Part of why she felt so bad was she had Covid! She got diagnosed because I got sick and tested positive. My 85 year old dad also caught it from her. The timeline shows she got it at the hospital and my dad and I got it from her. She is now housebound due to pulmonary edema and edema in her legs. She has fluid around the heart as well. She had heart issues beforehand so it’s amazing this hasn’t killed her. It may yet do so. She had been fully active before that hospital stay.
So no, Covid is not a cold.